
Gender Dysphoria and People with Intellectual Disability

Gender dysphoria has a very real impact on people’s lives. It is important that we acknowledge and respond to the needs of those with an intellectual disability who experience gender dysphoria
Ruth Bevan (UK) and Anna Laws (UK)
The gender continuum
Gender identity can be described as the private and subjective experience of one’s own gender, of maleness, femaleness, neither or both. Gender identity is diverse. We know that the “binary model”, of man or woman, boy or girl, does not fit many peoples’ experience of themselves. The spectrum model, whilst not the only valid model of gender, shows gender on a continuum (figure 1).
Society makes judgements about gender based on what individuals wear (gender expression), what they do (gender role) or even who they are attracted to (sexual orientation), but we must caution against such assumptions as they can often be wrong. Gender is a uniquely individual experience, one that no one can impose on another. Biological sex is generally considered to be binary but neither is this an accurate classification (Ainsworth, 2015).
Figure 1
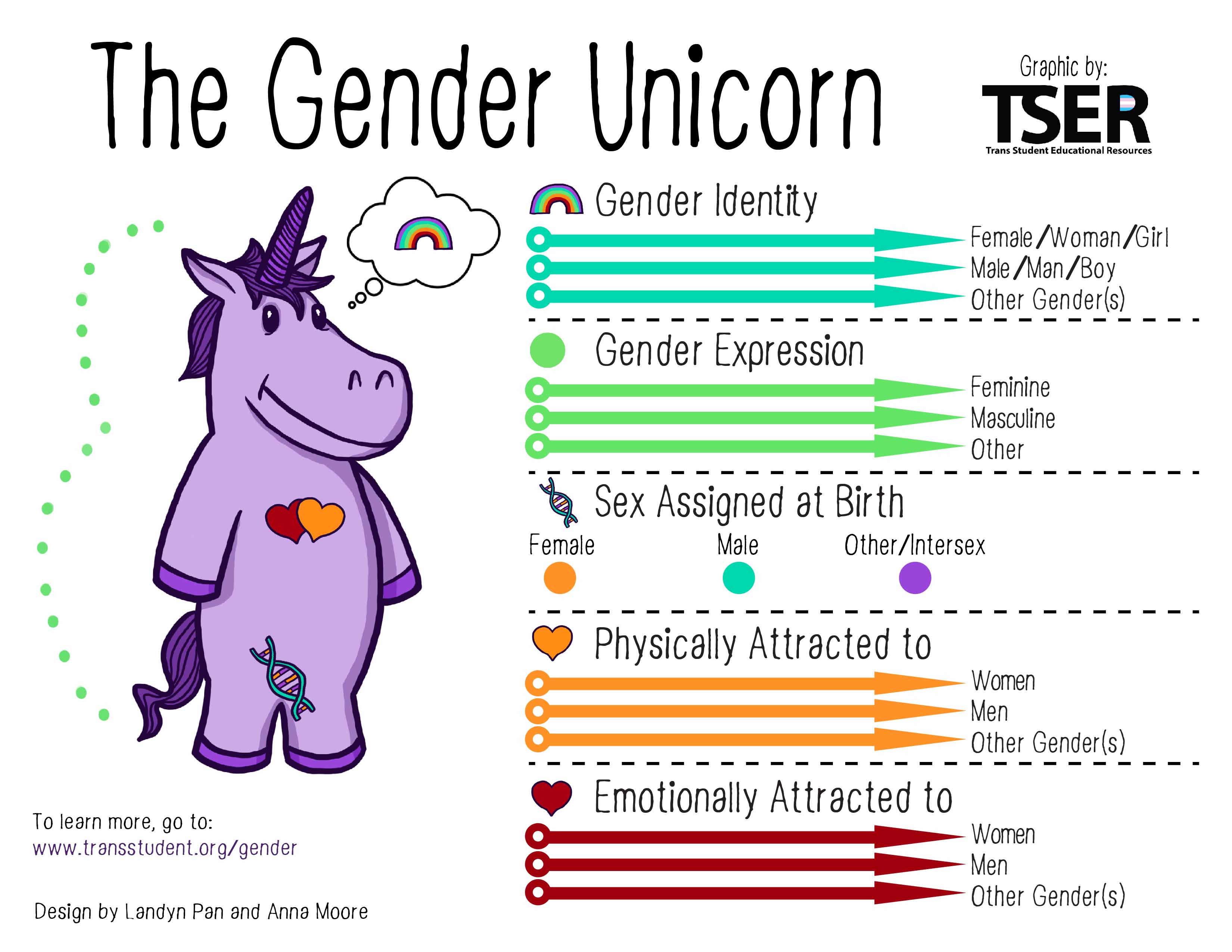
Source: http://www.transstudent.org/wp-content/uploads/2017/08/genderunicorn1.jpg
{kind=link}
Gender variance
Gender variance is when there is a difference between the sex that someone was assigned at birth and their experienced gender. For some, but not all, this variance can cause discomfort or distress. This is referred to as gender dysphoria. Gender dysphoria is classified diagnostically in DSM 5 as “Gender Dysphoria” and in ICD 10 as “Transsexualism”. ICD 11 adopts the term “Gender Incongruence”. Trans is an umbrella term which refers to all individuals who do not identify as a cisgender man or cisgender woman. Cisgender describes a person whose gender identity is the same as the sex that they were assigned at birth. Not everyone who identifies as trans experiences dysphoria.
Gender variance is not an uncommon phenomenon. The Equality and Human Rights Commission survey in 2012 found that 1% of the population experience gender variance. Gender identity clinics are seeing significant increases in referrals. People are presenting at an earlier age (Butler et al, 2018) and the gender difference is reducing with higher proportions of those assigned female at birth accessing services than in the past (Aitken et al, 2015). Gender variance exists everywhere, irrelevant of ethnicity, culture or socioeconomics, although it is more hidden in some societies.
Having a gender identity that does not conform to assigned sex is not a mental disorder and pathologising terms such as “gender identity disorder” should not be used. This is however an area that attracts interest and controversy. We often hear extremely polarising views about this subject. Trans individuals are frequently subjected to stigma, discrimination, rejection and abuse.
Intellectual disability and gender identity
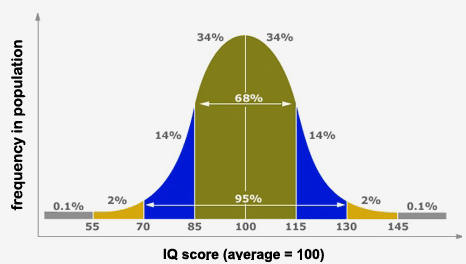
Here we see the normal distribution of IQ (figure 2). This portrays it as symmetrical with the area under the curve less than 70 equalling the area under the curve above 130. In reality we known that there are more at the lower end, due to biological or environmental influences which can act to bring IQ score down, and the numbers are increasing. Gender does not cease to exist below the point of 70. There are approximately 1.5 million people in the UK with an intellectual disability (https://www.learningdisabilities.org.uk/learning-disabilities/help-information/learning-disability-). If we use the estimated gender variance figure of 1%, this equals 15,000 individuals. We don’t have accurate statistics and prevalence rates of gender dysphoria in people with an intellectual disability are unknown. Some studies have suggested higher rates in people with an intellectual disability compared with those without, although there may be questions about methodology and small case numbers (Bedard et al, 2010).
Figure 2
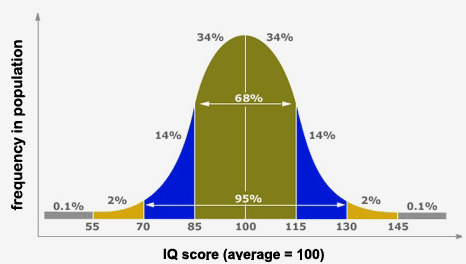
Source: http://www.highiqpro.com/wp-content/uploads/2012/03/IQ-Bell-Curve.png
{kind=link}
The gender milestone
Gender identity is influenced by biological, psychological and social variables. It develops through stages of increasing complexity. The achievement of an awareness of one’s own gender is a milestone. Abelson, in the late 1970s and 1980s studied this subject in a group of children with intellectual disability and autism spectrum disorder (Abelson, 1978). Using the Michigan GI test it was found that they too experienced a gender identity, and this formed a milestone, but having developmental delay impacted on when this milestone was achieved. Developmental disorders therefore may impact on development of gender identity, as well as other facets of identity such as personal and sexual identity. The impact of this will however vary considerably.
Gender and the autism spectrum
Whilst the focus of this article is on those with intellectual disability and gender dysphoria, it is important to acknowledge the coexistence of gender variance, intellectual disability and autism spectrum disorder (ASD) (figure 3). Studies in this area suggest higher rates of ASD, or ASD traits, in those referred to gender identity clinics (de Vries et al, 2010). This is supported by the clinical experience of those working in the field of gender dysphoria. Most of the published research focuses on children and young people with ASD with there being no prevalence studies in adults with a formal ASD diagnosis.
Figure 3
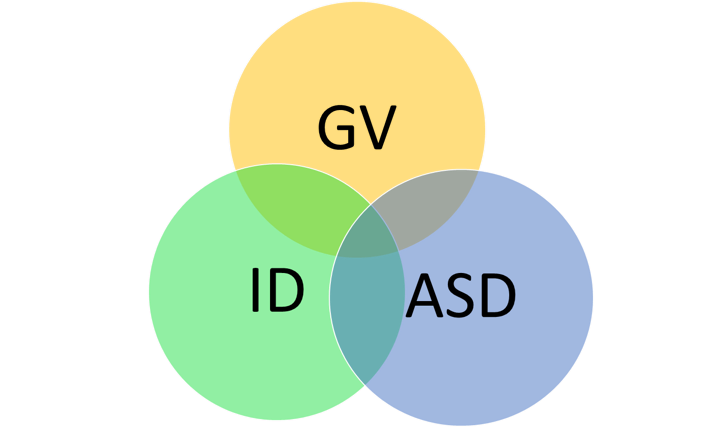
GV= gender variance ID= intellectual disability ASD= autism spectrum disorder
There are a number of the theoretical explanations given for higher rates of ASD. The extreme male brain theory puts forward the idea that a link between ASD and a more masculine gender identity, in those assigned female at birth, is due to high prenatal testosterone levels. This does not however account for the co-occurrence of gender dysphoria and ASD in those assigned male at birth. The potential for autistic traits to be associated with raised androgens, especially in those assigned female at birth, due to the effect of testosterone on the developing brain, has been hypothesised. Gender dysphoria could be seen as linked to obsessive interests, compulsions or preoccupations which present in those with ASD. The impact of lack of theory of mind on attachment, having implications for gender identity development, has been queried. Broader identity issues and a sense of not belonging, sometimes experienced by those with ASD, may mean they could be drawn to gender dysphoria as an explanation of their sense of being different. There are reports in the literature of young boys with an interest in feminine clothes and accessories, although such interests may more likely be linked to sensory needs rather than to gender identity.
These theories attempt to categorise individuals neatly and assumes that gender dysphoria is a manifestation of ASD. This may be unhelpful and distracts from the need for a broader view.
Another perspective is the idea that having ASD may mean that a person is less susceptible to external stimuli which reinforce social stereotypes or prejudices about gender. This may facilitate their ability to express their authentic self.
Clear conclusions about the links between gender dysphoria and ASD cannot be made. No specific guidelines to assist assessment and management in those with ASD currently exist and no studies report specific treatment outcomes. More research is needed in this area. A comprehensive review of this subject is available in Glidden et al, 2016.
Intellectual disability and gender dysphoria
Research looking at intellectual disabilities and gender dysphoria is limited to case studies and case series, mostly involving young people with ASD. There is no specific evidence base or guidelines to assist professionals working in this field. We know it exists and a wide range of learning abilities are described in the literature. In line with the general population, more people with an intellectual disability are presenting to gender identity clinics.
Some of the literature puts forward a number of possible reasons for people with intellectual disabilities presenting with issues related to gender such as: a means of escape, perhaps from life or their disability, to control anger, lack of fulfilling relationships or conflict arising from non-heterosexual orientation. Whilst it is important to assess these possibilities, we must also be willing to accept and embrace the idea that someone with an intellectual disability may have a trans identity.
Cognitive ability appears to influence how gender dysphoria presents. We may see more behavioural presentations as opposed to declarations. It is unlikely to present in individuals who are non-verbal, and given that the criteria relies on ability to express distress in relation to gender this is unsurprising. We see the influence of developmental delay on views of gender, gender role and sexuality with perhaps more rigidity in these ideas. Low self-esteem and lack of self-concept is a very important and under-acknowledged issue which is arguably worse in those with an intellectual disability. It is proposed that this may lead some to want to make changes to their identity. Role models play an important influence including those portrayed by the media. They provide ideas about what gender is and what different genders look like. These undoubtedly impact on the developing sense of self and are not always helpful.
It can be difficult for those familiar with the person to interpret what behaviours are communicative, hormonally driven or what may arise from dysphoria in these contexts. This is why we need services in place to support these individuals and those around them.
Those with an intellectual disability experiencing gender dysphoria can face a number of difficulties. Such individuals may not present the “classic” or “typical” history of gender dysphoria. However, this is the case for many people, with or without a developmental disorder. Having preconceived expectations about what we want to hear leads those whom we see feel pressure to give a history rather than their history. This does not help us help them and worse can be harmful.
Individuals may not give a history of gender dysphoria from early childhood. In those with intellectual disability it may be difficult to understand the chronology of their history and sequence of events. Many say they had no idea about gender as a concept, let alone what their own gender was, until they were older. How much of this could be due to the social impacts of a developmental disorder we don’t know.
The attitude and understanding of carers and families can have a significant effect on outcome. We know that those with support and easier access to services do better. There is a real risk that gender dysphoria goes unrecognised altogether in this group. Diagnostic over-shadowing means that there is a single diagnosis driving the overall view. In society there is a tendency to infantilise people with an intellectual disability even when they are adults. We need to recognise and challenge this when we see it. Occasionally individuals describing a clear trans identity can sometimes be described by others as “confused”. We must be careful not to interpret gender variance as confusion. The environment can impact significantly. There may be practical limitations such as access to transport and finances. Limited autonomy means that individuals are reliant on others to have many of their needs met.
We must not forget that those with developmental disorders such as intellectual disability may have additional mental and physical health needs which can impact on assessment and treatment plans. These can sometimes be used to prevent individuals from accessing support and assessment, despite guidelines advocating access to treatment for gender dysphoria (CR 181, 2013). It is widely recognised that treatment for gender dysphoria has far-reaching benefits.
When working with people with an intellectual disability effective communication is vital. Even if an individual is able to communicate competently on a day-to-day basis, within their ordinary environment and routines, many will have significant communication difficulties which may become unmasked during unfamiliar or more complex discussions. Individuals may have a rich and varied vocabulary but words may not be used accurately or appropriately. Access to previous speech and language reports and cognitive assessments can be crucial to enable understanding and supporting of these needs.
We must appreciate the impact of an individual’s emotional state. Anxiety, excitement, heightened states of arousal and sensory overload are unlikely to promote effective communication. Individuals may themselves be unaware that they are struggling with their communication. They may feel and indicate that a task has gone well when it hasn’t. Individuals will often be keen to “get things right” and to please the professional.
An important part of assessment in those with an intellectual disability involves helping someone to explore their gender identity by thinking and talking about it. People may need reassurance to do this openly without fear of ridicule or potential consequences. This exploration shouldn’t be confined to the clinic room. People need to continue this outside, in their homes and communities. This may be met with barriers. Simple scrapbook exercises to do at home with family/carers can be helpful. Rigid ideas about gender, gender roles and sexuality need to be challenged and broadened. Using examples from within someone’s own experience can be helpful in doing this.
It is important to discuss expectations as these may be unrealistic and unfulfillable and can lead to disappointment. Such discussions need to be frank.
Gender identity clinics must work collaboratively with patients, their families and carers. It is vital to involve other services and professionals relevant to the individual. Frequently additional training is required. Assessment and treatment pathways can therefore be lengthy and resource consuming.
Safeguarding
We must always consider a person’s well-being and safety. Sadly for some of the individuals safeguarding concerns may be raised. This can be for a variety of reasons such as:
- An individual is prevented from socially transitioning, or accessing assessment and treatment.
- Risks associated with transphobia.
- Misperception/ misattribution, for example, viewing behaviour as “sexually deviant” or “fetishistic”.
- The pressure to keep secret the wish to wear certain clothes, or denying access to such items, may mean an individual has to resort to stealing them.
- Occasionally concerns are raised that individuals may be under the influence of others or are being coerced.
- Other trans specific vulnerabilities. For example, the hormones prescribed have a street value and can be misappropriated.
Capacity
The issue of capacity is often raised. Mental capacity refers to being able to make your own decisions. What information does one need to understand, retain, weigh up or use to decide one’s gender identity?
Gender identity is a private and subjective experience, not a decision to be made. We would never ask a cisgender person to justify theirs therefore questioning capacity in this regard is inherently discriminatory. Decisions may arise further on in regard to aspects of social transition or informed consent to treatment. Decision-making about medical management is usually more straightforward. Decisions about social management can be more complex. Some of these decisions may involve other people such as family, carers and other professionals. It is important to remember people are allowed to make, what others may deem to be, unwise decisions. If an individual is deemed not to have capacity decisions should be made based on best interest. Failing to support a person to express their gender identity is not a risk free position.
Summary
Gender dysphoria has a very real impact on people’s lives. The messages we receive about this issue are often extreme and polarising. Here we have considered the problems which may exist for this group. However whilst there are many challenges, negative experiences are not universal.
Whilst we lack specific outcome data for these groups, clinical consensus indicates that treatment can have significant benefits in reducing distress and also broader outcomes such as improved social communication and functioning.
It is important that we acknowledge and respond to the needs of those with an intellectual disability who experience gender dysphoria. We should remain open minded about how it may present and listen to the story the person tells, without making quick and obvious assumptions or judgements due to the pressure to make a definitive or singular diagnosis, or because of our own anxiety about where this could lead.
We must be careful not to make having a developmental disorder a further barrier to accessing help but listen, learn and better understand so that we can help such individuals be their authentic and best.
Useful links
https://www.itspronouncedmetrosexual.com/
References
Abelson G. (1978). Gender Identity in a Group of Retarded Children. Journal of Autism and Childhood Schizophrenia, 8(4): 403-411
Ainsworth, C., 2015. Sex redefined. Nature News, 518(7539), p.288.
Aitken, M., Steensma, T.D., Blanchard, R., VanderLaan, D.P., Wood, H., Fuentes, A., Spegg, C., Wasserman, L., Ames, M., Fitzsimmons, C.L. and Leef, J.H., 2015. Evidence for an altered sex ratio in clinic‐referred adolescents with gender dysphoria. The journal of sexual medicine, 12(3), pp.756-763.
Bedard, C., Zhang, H.L. and Zucker, K.J., 2010. Gender identity and sexual orientation in people with developmental disabilities. Sexuality and Disability, 28(3), pp.165-175.
Butler, G., De Graaf, N., Wren, B. and Carmichael, P., 2018. Assessment and support of children and adolescents with gender dysphoria. Archives of disease in childhood, 103(7), pp.631-636.
College Report 181 (2013). Good practice guidelines for the assessment and treatment of adults with gender dysphoria. Royal College of Psychiatrists
De Vries, A.L., Noens, I.L., Cohen-Kettenis, P.T., van Berckelaer-Onnes, I.A. and Doreleijers, T.A., 2010. Autism spectrum disorders in gender dysphoric children and adolescents. Journal of autism and developmental disorders, 40(8), pp.930-936.
Glidden, D., Bouman, W.P., Jones, B.A. and Arcelus, J. (2016). Gender dysphoria and autism spectrum disorder: A systematic review of the literature. Sexual Medicine Reviews, 4(1), pp.3-14
This article was first published on this site in 2019