
Embodiment, learning and wellbeing
Professor Helen Payne, PhD, University of Hertfordshire

Introduction
Embodiment is concerned with the body as who we are, the subjective, body-felt sense from the inside-out - a first person perspective and the application can be to wellbeing, relationships, leadership, psychotherapy, education, etc. In the medical model the body is viewed as an object - a third person perspective. First person experience is usually considered to need validation whereas scientific understanding is privileged.
The embodied paradigm views mind, which is not only the brain (Siegal, 2007, 2015), and body as inseparable, having a bi-directional relationship as opposed to being disconnected as in conventional Cartesian dualistic thinking which views body and mind as isolated from each other. Scans of the brain when people think /imagine things or meditate, show changes in blood-flow, neurotransmitter and electrical activity in the brain. Therefore, for any subjective act there is a physical basis. Mental activity affects the brain and the body but what about vice-versa?
Emotions and the body
As far back as Darwin (1872), James (1884) and Lange (1885) who independently suggested the origins of emotional feeling occurs as a result of bodily responses to events i.e. an external stimulus leads to a physiological reaction. Emotions held in the body make, for example, the fight-flight-faint-freeze-fold stress responses. Laird (1974) found when people are made to smile (holding a pen between their teeth) they become happier and when asked to ‘nod’ are more likely to agree.
Porges (2009) showed how the polyvagal theory illustrates reciprocal influences between body and brain in the perception and expression of affect. Wiseman (2012) suggests personal development is ineffective with positive thinking but effective when conducted with physical action. Research by Zhong et al., (2010) discovered people who carried out an immoral act and then cleaned their hands with an antiseptic wipe felt significantly less guilty than others. Findings by Hung and Labroo (2011) showed willpower is linked to contracting muscles. Lakoff (2012) observed leaning forward stimulates desire and purpose. Heavier books are judged as more important. (ibid: 782). People judge a neutral stranger as more generous and caring when holding a warm versus cold beverage (Williams and Bargh, 2008). Furthermore, Ackerman et al. (2010) found participants sitting on soft or hard chairs showed differences in negotiation styles.
Social judgments such as friendliness, threat and intimacy are embodied. Positive evaluations of a demographic group (the elderly) unconsciously mimicked their movement patterns (slower gait) (Cesario, Plaks, and Higgins, 2006). Social psychology research increasingly illustrates the myriad ways in which social interactions and behaviour are embodied (Niedenthal, Barsalou, Winkielman, Krauth-Gruber, and Ric, 2005).
Postures corresponding with certain mental and emotional states are used in the somatic therapies such as dance movement psychotherapy (DMP) (Duclos and Laird, 2001; Carney et al., 2010; Shafir et al., 2013, 2016; Koch, 2014; Koch et al., 2014). This link goes both ways. Not only can being depressed, for example, make us slump and our facial expressions change, but slumping and changing our facial expressions can make us depressed as actors already know (Ekman, 1971). Shafir (2015; 2016) found movement could regulate emotions by the deliberate control of motor behaviour and the consequent proprioception and interoception affecting feelings as used in DMP. Here clients may be guided to move in a certain way helping them to experience, process, and regulate specific emotions contributing to emotional regulation.
Research on the connection between movement style and personality type such as North (1972) has been common for almost half a century. More recently, Luck et al., (2010) used movement and postural patterns to judge personality as did Koppensteine (2013). Reich (1980) proposed character styles from reading bodies and their tension patterns and Laban (1950) observed the personal kinesphere (the space into which one can reach around one’s body) and effort (the quality of movement) combinations to illustrate states of mind. Motion capture technology can offer a valid video psychometric helping to distinguish between projection of stereotypes and accurate assessments.
Embodied cognition
Traditional understanding is that knowledge is represented abstractly in an amodal (perception of the whole of a physical structure e.g. a chair, when only parts of it may affect the sensory receptors) or supramodal (referring to an area of the brain implementing abstract functionality common to more than one source of sensory data e.g. the areas concerned with language processing can integrate data from visual, auditory and tactile areas of the brain) conceptual network of formal logic symbols (Fodor, 1975).
Embodied cognition challenges this view claiming cognitive representations that constitute our knowledge are grounded in both sensory and motor experiences (Lakoff & Johnson, 1999; Barlsalou, 2008). Varela et al. (1992, 172-3) define ‘embodied’ to mean that ‘cognition depends upon the kinds of experience that come from having a body with various sensorimotor capacities’ and that individual sensorimotor capacities are embedded in a biological, psychological and cultural context. From applications in philosophy (Gallagher, 2005) and robotics (Paradowski, 2012), for example, embodied cognition states thinking is dependent on bodily feedback and the environment (Lakoff & Johnson, 1999). This view has implications for both psychotherapy and education (for example, pedagogy).
Consequently, it can be claimed change in body states changes thinking and behavioural tendencies i.e. environmental and a habitual personality influenced body state is the substrate of thinking, perceiving, acting, relating etc. Managing states through practices involving posture, movement, breathing, visualisation and awareness are basic tools in embodied approaches which can be employed in psychotherapy, mental health care and learning and teaching settings. Despite embodiment only just gaining recognition in the public domain, after being ignored, it has a rich history as a concept.
Embodiment and learning
Damasio et al., (2000) and Damasio and Carvello (2013) have shown emotions are generated by conveying the state of the body to the brain through interoceptive and proprioceptive afferent input. The resulting patterns of brain activation represent unconscious emotions which correlate with conscious feelings. Mirror neurons have a role in embodied simulation (Gallese & Sinigaglia, 2011) creating in the observer an internal simulation of movements observed, which lead to the same emotions being felt in the observer as expressed by the observed moving person (Niedenthal, 2007; Heberlein and Atkinson, 2009). This embodied simulation occurring during motor observation is the basis for emotional empathy (Nummenmaa et al., 2008; Decety, 2011) and is the underlying mechanism in movement analysis and the practice of authentic movement when employed in psychotherapy (Payne, 2017). Cultivating embodied empathy, such as practices beyond mindfulness ((Kabat-Zinn, 2003), could improve, for example, supportive relationships, compassion and ‘presence’ in teaching and psychotherapy.
Neuroscience therefore provides evidence to the embodied learning approach, such as the impact of implicit procedural learning and the importance of conscious practice to overcome engrained circuitry and habits. Reading is insufficient to change behaviour as we are neurologically inclined to certain emotionally linked behaviours. Neuroscience studies show how the amygdala can ‘hijack’ the brain, effectively turning off the neocortex, as in fight/ flight stress responses, necessitating practices such as centring to regain the use of more rational neocortical areas of the brain. Neuroscience describes how the heart and gut have large numbers of neurones, sometimes even called secondary brains, relevant to embodied learning. Nerves are distributed throughout the body and our whole nervous system is linked together making the whole body a brain. Neuroscience highlights the social relational nature of the human nervous system and why learning through interaction and community found in embodied approaches is so powerful. Note the neglect demonstrated by the Romanian orphans for whom the ill effects without the presence of touch, movement and social connectiveness were shocking (Rutter et al., 1998). Insights from research in neuroscience may aid the design of teaching and learning strategies, for example, promoting interaction between learners within a cohesive group, strong alliances, a supportive climate and explicitly shared goals. Additionally, ensuring the learning and teaching environment is safe and stress-free for all which may contribute to emotional-regulation, more effective learning and improved outcomes.
Embodied approaches to wellbeing
Together with the talking therapies and the arts therapies (the latter employing creativity from an arts-based and aesthetics perspective as an embodied approach to psychotherapy for promoting mental health and wellbeing) there are many other activities which enable wellbeing. Some, for example, are through the body, including martial arts, yoga, fitness regimes, walking, etc. Certainly, physical wellbeing is part of promoting good wellbeing and mental health.
However, some bodily symptoms may serve to prevent such physical activities, for example, those for which tests and scans always come back negative (fibromyalgia, chronic pain, IBS, or chronic fatigue etc.) called medically unexplained symptoms (MUS). Mindfulness might be an alternative to a more physical engagement for wellbeing since the evidence demonstrates it has an impact on reducing stress (Kabat-Zinn, 2003, 2005b) and chronic pain (Kabat-Zinn, 2005a). Furthermore, there is evidence that mindfulness can reduce the often, co-occurring depression and anxiety (Hofmann, Sawyer, Witt, & Oh, 2010) and have a moderate effect on some MUS (Grossman, Niemann, Schmid, & Walach, 2004). There is also an association between lack of mindful self-awareness and depression (Segal, Williams & Teasdale (2002). This lack of self-awareness results in poor recognition and reflection on bodily cues or signals such as tension, pain, fatigue, destructive patterns, negative thoughts or feelings. Mindful self-awareness can help a dis-identification with bodily symptoms which are so often tied up with identity for people with MUS (Sanders, Winter & Payne, 2018).
However, mindfulness does ignore practice from an embodied platform. Our bodies are designed for movement/action and it has been shown that practices beyond mindfulness such as gentle body awareness exercises or somatic mindfulness sometimes referred to by the author as ‘body mindfulness’ can enhance and sustain well-being which is particularly helpful for people distressed by such chronic bodily symptoms, many of which can increase stress levels resulting in even more bodily distress and some even caused by the stress in the first place.
By learning to be aware of any ‘somatic marker’ (Damasio, 1999) which can be used as an early warning signal of a habitual stress response kicking in, a protective function can be put in place to buffer against the symptoms becoming worse. Through mindfully being in the ‘movement moment’, for example, noticing how much push from the heel there is when you walk, (illustrating perhaps a need for more ‘push’ to improve confidence levels) facilitates an internal (interoceptive) awareness during action thereby cultivating learning to take account of the aforementioned body signals. The BodyMind Approach® (TBMA) for supporting people with MUS to learn how to self-manage has been designed specifically with this above research in mind (Payne, 2015, 2016, 2017; Payne & Brooks, 2018, 2019).
The BodyMind Approach®: The Outcomes
TBMA is based on research (for example, see Payne, 2010) and is also a research-informed intervention designed in structure and content to take account of research in neuroscience, embodied and transformational adult learning, group work, safety, self-regulation, attachment and mindfulness. Consequently, TBMA has been conducted as research-informed practice, as well as evidence-based practice and practice-based evidence (Payne & Stott, 2010; Payne & Brooks, 2017; 2018, 2019). From deliveries in the NHS over 90 patients mirrored the original research outcomes. A TBMA study of women with/without depression with MUS in Taiwan (Lin, 2016, Lin & Payne, 2018) (N=24) also demonstrated a significant reduction in symptom distress.
Reliable change outcomes from a county-wide NHS delivery[1] showed 73% of people who engaged in TBMA programmes with different TBMA certified facilitators reported lower levels of:
- symptom distress
- anxiety
- depression
and higher levels of:
- wellbeing
- overall functioning
- activity
This data was drawn from the 95% of people who completed the TBMA groups. Additionally, pre to post course analysed for reliable change demonstrated for depression and anxiety showed:
- Depression 35% improvement alone
- Anxiety 42% improvement alone
To avoid double counting it is necessary to exclude people who improved on both measures. Thus, figures used to calculate the percentage are less than combining the two figures giving a Depression + Anxiety overlap score of 65%. Many participants were medicated for depression and/or anxiety and most MUS suffered mild to moderate depression/anxiety. Depression and/or anxiety however are not the presenting problem nor what people appear to be most concerned about which are their symptoms. Overall there was very little reliable deterioration.
Furthermore, a Participant Experience Form distributed post group, of which 97% completed, showed 70% felt they had enough help to go forward. The initial contact, assessment telephone monitoring, group experience/content, facilitator and overall service were rated as ‘satisfactory’ to ‘very satisfactory’ and 79% would use the service again without hesitation whereas 97% would recommend the service to friends and family without hesitation. Table 1 below demonstrates the improvement in not only day today self-management of symptoms but also coping with them at work from pre to post course intervention for those to whom we directed and answered this question.
| Before course | After course | |
|---|---|---|
| Coping well with symptoms | 4% (1/24) | 52% (12/23) |
| Coping well at work | 14% (3/22) | 50% (11/22) |
Figure 1: To show the effect of participants’ symptoms on ability to work
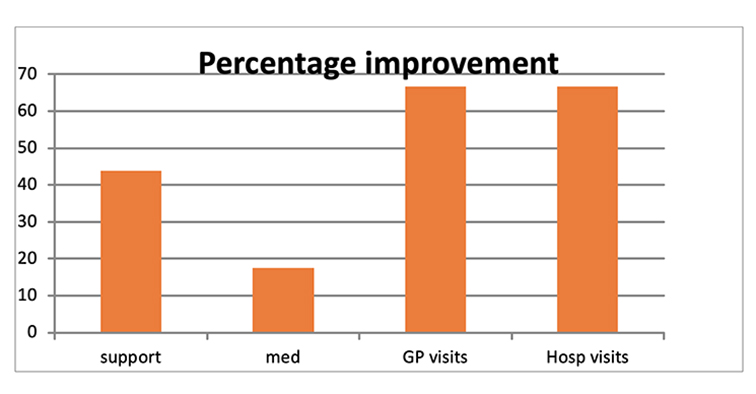
Figure 2: Percentage improvement in social support, medication, GP & hospital visits pre to post course
Table 2 above shows the percentage of people who reported they did not need to return to hospital, or the GP, their social support improved and for a few, medication reduced from pre to post TBMA workshops. The six-month follow up analysis compared to post group showed improvements not only sustained at three months post group (as in the original study) but were maintained/improved further at the six-month stage in: functioning; wellbeing; anxiety; depression and symptom distress. The six-month follow up compared to pre-group analysis showed:
- Improvement or maintenance of activity levels (50% of people becoming more active /50% remaining the same when compared to pre-group).
- Improved well-being maintained in 50% of people at post-group when compared to pre- group.
- Improvement in social, occupational and overall functioning in 75% of people when compared to pre-group.
Conclusion
It can therefore be cautiously concluded most participants report important improvements in their perception of their symptoms which helps them to self-manage their conditions and consequently cope better day to day (supported by the quantitative data). Participants demonstrate their capacity for resilience post TBMA intervention, self-management becomes habitual, feelings of wellbeing are sustained, empowerment is cultivated to control symptoms over time and there is a reduced dependence on the NHS (an economic argument).
Reliable change outcomes have been demonstrated whereby TBMA promotes the self-management of symptoms by employing embodied learning practices resulting in participants blossoming having learned to competently self-manage their symptoms day-to-day.
Adopting a research-informed embodied approach to learning in education policy and/or practices might raise awareness of the benefits of embodied learning (which is broadly already employed in physical education, technologies, the arts and sciences as they are practical subjects), for other subjects in educational institutions. To cultivate learners to blossom active, socially interactive learning approaches could be designed in preference to the conventional learning arrangement often found at all levels of education of sitting in stillness with engagement through visual methods. Pedagogy might consider how learning takes place, i.e. through body, mind, and brain.
[1] These outcomes have been published previously in Payne, H., & Brooks, S. D. M. (2017). Moving on: The BodyMind Approach for medically unexplained symptoms. Journal of Public Mental Health, 16(2), 1-9.
References
Ackerman, J. M., Nocera, C. C. and Bargh, J. A. (2010). Incidental haptic sensations influence social judgments and decisions. Science, 328, 1712–1715, https://doi.org/10.1126/science.1189993.
Barsalou, L. W. (2008). Grounded cognition. Annual Review of Psychology 59, 617–645.
Carney, D. R., Cuddy, A. J. C., and Yap, A. J. (2010). Power posing brief nonverbal displays affect neuroendocrine levels and risk tolerance. Psychological Science, 21, 1363–1368. doi: 10.1177/0956797610383437
Cesario, J., Plaks, J. E., and Higgins, E. T. (2006). Automatic social behavior as motivated preparation to interact. Journal of Personality and Social Psychology, 90(6), 893–910.
Damasio, A.R. (1999). The feeling of what happens: Body and emotion in the making of consciousness. New York, NY: Houghton Mifflin Harcourt.
Damasio, A., and Carvalho, G. B. (2013). The nature of feelings: evolutionary and neurobiological origins. Nat. Rev. Neuroscience, 14, 143–152. doi: 10.1038/nrn3403
Damasio, A. R., Grabowski, T. J., Bechara, A., Damasio, H., Ponto, L. L. B., Parvizi, J., et al. (2000). Subcortical and cortical brain activity during the feeling of self-generated emotions. Natural Neuroscience, 3, 1049–1056. doi: 10.1038/79871
Darwin, C. R. (1872). The expression of the emotions in man and animals. London: John Murray.
Decety, J. (2011). Dissecting the neural mechanisms mediating empathy. Emotion Review, 3, 92–108. doi: 10.1177/1754073910374662.
Duclos, S. E., and Laird, J. D. (2001). The deliberate control of emotional experience through control of expressions. Cognitive Emotion. 15, 27–56. doi: 10.1080/0269993004200088
Ekman, P. (1971). Universals and cultural differences in facial expressions of emotion. Nebraska Symposium on Motivation, 19, 207-283.
Fodor, J. A. (1975) The language of thought. Cambridge, USA: Harvard University Press.
Gallese, V., and Sinigaglia, C. (2011). What is so special about embodied simulation? Trends Cognitive Science. 15, 512–519. doi: 10.1016/j.tics.2011.09.003
Gallagher, S. (2005). How the body shapes the mind. Oxford: Oxford University Press.
Grossman, P., Niemann, L., Schmid, S., and Walach, H. (2004). Mindfulness-based stress reduction and health benefits: A meta-analysis. Journal of Psychosomatic Research. 57:35–43.
Heberlein, A. S., and Atkinson, A. P. (2009). Neuroscientific evidence for simulation and shared substrates in emotion recognition: beyond faces. Emotion Review. 1, 162–177. doi: 10.1177/1754073908100441
Hofmann, S. G., Sawyer, A. T., Witt, A. A., Oh, D. (2010). The Effect of mindfulness-based therapy on anxiety and depression: A meta-analytic review. Journal of Consult Clinical Psychology, April; 78(2): 169–183. doi: 10.1037/a0018555.
Hung, I. W., Labroo, A. A. (2011). From firm muscles to firm willpower: Understanding the role of embodied cognition in self-regulation. Journal of Consumer Research. 37(6): 1046–1064. doi:10.1086/657240. ISSN 0093-5301.
James, W. (1884). What is an emotion? Mind, 9, 188–205. doi: 10.1093/mind/os-IX.34.188.
Kabat-Zinn, J. (2003). Mindfulness-based interventions in context: past, present and future. Clinical Psychology: Science and Practice, 10, 2, 133-156.
Kabat-Zinn, J. (2005a). Full catastrophe living: Using the wisdom of your body and mind to face stress, pain, and illness: Fifteenth anniversary edition. New York: Bantam Dell.
Kabat-Zinn, J. (2005b). Coming to our senses: Healing ourselves and the world through mindfulness. New York: Hyperion.
Koch, S. C. (2014). Rhythm is it: effects of dynamic body feedback on affect and attitudes. Frontiers in Psychology. 5:537. doi: 10.3389/fpsyg.2014.00537
Koch, S. C., Fuchs, T., and Summa, M. (2014). Body memory and kinesthetic body feedback: the impact of light versus strong movement qualities on affect and cognition. Memory Studies, 7, 272–284. doi: 10.1177/1750698014530618
Koppensteine, M. (2013) Motion cues that make an impression: Predicting perceived personality by minimal motion information. Journal of Experimental Social Psychology 49, 1137–1143.
Laban, R von. (1950). The mastery of movement on the stage. London: MacDonald & Evans
Lakoff, G (2012) Explaining Embodied Cognition Results. Topics in Cognitive Science, 4, 4, https://doi.org/10.1111/j.1756-8765.2012.01222.x
Lakoff, G. and Johnson, M. (1999). Philosophy in the flesh: The embodied mind and its challenge to western thought. New York, NY: Basic Books.
Laird, J. D. (1974). Self-attribution of emotion: The effects of expressive behavior on the quality of emotional experience. Journal of Personality and Social Psychology 29 (4): 475–486. doi:10.1037/h0036125.
Lange, C. (1885) The emotions. Baltimore: Williams and Wilkins.
Lin, Y. C. (2016) Cultural-related depression in Taiwanese women and the application of The BodyMind Approach. Submitted in partial fulfilment of a PhD, University of Hertfordshire. Unpublished.
Lin, Y.C. and Payne, H. (2018). Movement speaks of culture: A study focusing on women with depression in Taiwan. The Arts in Psychotherapy, accepted 30/11/18. Published online.
Luck, G., Saarikallio, S., Burger, B., Thompson, M. R., and Toiviainen, P. (2010). Effects of the Big Five and musical genre on music-induced movement. Journal of Research in Personality, 44, 714-720, 10.1016/j.jrp.2010.10.001.
Niedenthal, P. M. (2007). Embodying emotion. Science, 316, 1002–1005. doi: 10.1126/science.1136930
Niedenthal, P. M., Barsalou, L. W., Winkielman, P., Krauth-Gruber, S., and Ric, F. (2005). Embodiment in attitudes, social perception, and emotion. Personality and Social Psychology Review, 9 (3), 184–211.
Nummenmaa, L., Hirvonen, J., Parkkola, R., and Hietanen, J. K. (2008). Is emotional contagion special? An fMRI study on neural systems for affective and cognitive empathy. Neuroimage, 43, 571–580. doi: 10.1016/j.neuroimage.2008.08.014
North, M (1972) Personality assessment through movement. London: MacDonald and Evans.
Paradowski, M. B. (2012). Developing embodied multisensory dialogue agents. In R. Rzepka, M. Ptaszyński and P. Dybala (Eds.), Linguistic and cognitive approaches to dialogue agents. (p 6-14). Birmingham: The Society for the Study of Artificial Intelligence and Simulation of Behaviour.
Payne, H., and Stott, D. (2010). Change in the moving bodymind: Quantitative results from a pilot study on the BodyMind Approach (BMA) to group work for patients with medically unexplained symptoms (MUS). Counselling and Psychotherapy Research, 10, 4, 295-307.
Payne, H. (2015). The Body speaks its mind: The BodyMind Approach for patients with medically unexplained symptoms in the UK primary care health system. The Arts in Psychotherapy, 42, 19-27.
Payne, H. (2016). Clinical outcomes from The BodyMind Approach in the treatment of patients with medically unexplained symptoms in the English primary care setting: Practice-Based Evidence. The Arts in Psychotherapy, 47, 55-65.
Payne, H (2017) The psycho-neurology of embodiment with examples from Laban Movement Analysis and Authentic Movement. American Journal of Dance Therapy, online 7th June, 2017. DOI 10.1007/s10465-017-9256-2
Payne, H., and Brooks, S. D. M. (2017). Moving on: The BodyMind Approach for medically unexplained symptoms. Journal of Public Mental Health, 16(2), 1-9.
Payne, H. (2018). The BodyMind Approach: Supporting the wellbeing of patients with chronic medically unexplained symptoms in primary health care in England. In: V. Karkou, Vicky, S. Oliver, S. Lycouris (Eds.), The Oxford Handbook of Dance and Wellbeing. (pp769-789). Oxford: Oxford University Press.
Payne, H., and Brooks, S. (2018). The BodyMind Approach for patients with medically unexplained symptoms to learn to self-manage, Frontiers in Psychology, section Clinical and Health Psychology, Open Access. http://journal.frontiersin.org/article/10.3389/fpsyg.2018.02222/full?&utm_source=Email_to_authors_&utm_medium=Email&utm_content=T1_11.5e1_author&utm_campaign=Email_publication&field=&journalName=Frontiers_in_Psychology&id=371037
Payne, H., and Brooks, S. (2019). A theory of embodied learning for self-management: A qualitative analysis of patient perceptions of The BodyMind Approach for people with medically unexplained symptoms (in preparation).
Porges, S.W. (2009). Reciprocal influences between body and brain in the perception and expression of affect: A polyvagal perspective. In: D. Fosha and D. J. Siegel (Eds.). The Healing Power of Emotion: Affective Neuroscience, Development and Clinical Practice (pp. 27-54). New York: NY: W.W. Norton and Co.
Reich, W. (1980). Character analysis. Farrar, Straus & Giroux Inc; 3rd ed. Edition.
Rutter, M., and the English and Romanian Adoptees (E.R.A.) Study Team. (1998). Developmental catch-up, and deficit, following adoption after severe early privation. Journal of Child Psychology and Psychiatry, 39, 465 – 476.
Sanders, T., Winters, D., and Payne, H. (2018). Personal constructs of mind-body identity in people who experience medically unexplained symptoms (MUS). Journal of Constructivist Psychology, online August 2017.
Segal, Z. V., Williams J. M. G., and Teasdale, J. D. (2002). Mindfulness-based cognitive therapy for depression: A new approach to preventing relapse. New York: Guilford Press.
Siegel, D. J. (2007). The mindful brain: reflection and attunement in the cultivation of well-being. New York: W. W. Norton & Company.
Siegal, D. J. (2015). The developing mind: How relationships and the brain interact to shape who we are. Second edition. Gilford Press.
Shafir, T. (2015). Movement-based strategies for emotion regulation. In M. L. Bryant (Ed.), Handbook on Emotion Regulation: Processes, Cognitive Effects and Social Consequences, (p 231–249). New York, NY: Nova Science Publishers, Inc.
Shafir, T. (2016) Using movement to regulate emotion: Neurophysiological findings and their application in psychotherapy. Frontiers in Psychology, 23 September, https://doi.org/10.3389/fpsyg.2016.01451.
Shafir, T., Tsachor, R. P., and Welch, K. (2016). Emotion regulation through movement: unique sets of movement characteristics are associated with and enhance basic emotions. Frontiers in Psychology, 6:2030. doi: 10.3389/fpsyg.2015.02030
Shafir, T., Taylor, S. F., Atkinson, A. P., Langenecker, S. A., and Zubieta, J.-K. (2013). Emotion regulation through execution, observation, and imagery of emotional movements. Brain Cognition. 82, 219–227. doi: 10.1016/j.bandc.2013.03.001
Varela, F. J., Rosch, E., and Thompson, E. (1992). The Embodied Mind: Cognitive science and human experience. (p172–173). Cambridge, Mass: MIT Press.
Williams, L. E., and Bargh, J. A. (2008). Experiencing physical warmth promotes interpersonal warmth. Science, 322 (5901), 606–607.
Wiseman, R. (2012). Rip it up: The radically new approach to changing your life. London: Macmillan.
Zhong, C., Strejcek, B., and Sivanathan, N. (2010). A clean self can render harsh moral judgment. Journal of Experimental Social Psychology, 46 (5), 859-862 DOI: 10.1016/j.jesp.2010.04.003